 |
Knee osteoarthritis can progress slowly over years. Some patients manage symptoms with exercise, medication, injections, weight loss, bracing, or physical therapy. Others eventually reach a point where knee replacement becomes the best option.
But many people fall somewhere in between.
They have real pain. They have limitations. They may have already tried conservative treatments. But they are not ready for knee replacement, do not want surgery yet, or have health concerns that make surgery more complicated.
That is where Genicular Artery Embolization, or GAE, may enter the conversation.
GAE is not “better than” knee replacement, and it is not a replacement for orthopedic care. It is a minimally invasive treatment option that may help selected patients with knee osteoarthritis pain who are looking for another step before surgery.
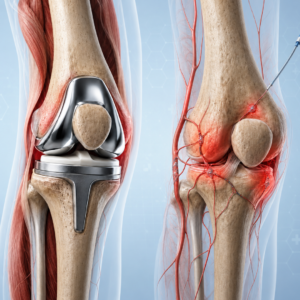 |
Knee replacement is a surgical procedure that removes damaged joint surfaces and replaces them with artificial components. For patients with advanced arthritis and severe structural damage, knee replacement can be an important and appropriate treatment.
GAE works differently. It does not remove or replace the joint. Instead, it targets abnormal blood vessels around the knee that may contribute to inflammation and pain in osteoarthritis. UCLA Health notes that knee replacement is the definitive treatment for knee osteoarthritis, while GAE may serve as a minimally invasive option for patients who are not quite ready for knee replacement and are relying on medications, injections, or other nonsurgical treatments with variable success.
GAE may be considered for patients who have knee osteoarthritis pain that continues despite conservative treatment, want to delay knee replacement, are not good surgical candidates, or prefer to explore a minimally invasive option first.
A GAE evaluation may also be appropriate for patients who have been told they are “not bad enough” for knee replacement but still have pain that interferes with walking, exercise, work, travel, or daily activities.
The decision should be individualized. Your vascular specialist may coordinate with your orthopedic physician, primary care provider, physical therapist, or pain management clinician to understand your full treatment history and goals.
GAE is designed to reduce pain related to inflammation around the knee. For the right patient, the goal is less pain, better function, and improved quality of life.
However, it is important to have realistic expectations. GAE does not grow new cartilage, straighten a severely deformed knee, repair ligaments, or guarantee that knee replacement will never be needed. Some patients may still need orthopedic surgery later.
This is why patient selection matters. The Society of Interventional Radiology emphasizes that GAE should be performed in appropriately selected patients and within a multidisciplinary care model.
 |
A consultation is the best way to understand whether GAE fits your situation. Useful questions include:
What is likely causing my knee pain?
Have I tried the right conservative treatments?
Does my imaging suggest osteoarthritis?
Am I a candidate for GAE?
Would I still be able to have knee replacement later if needed?
What are the risks, benefits, and recovery expectations?
Your physician should explain where GAE fits in your overall knee care plan.
GAE and knee replacement are not the same treatment. Knee replacement addresses advanced joint damage surgically. GAE is a minimally invasive procedure that may help selected patients manage osteoarthritis-related knee pain before surgery becomes necessary or appropriate.
If you have chronic knee pain and want to understand your options, contact Heart Vascular & Leg Center to schedule a GAE consultation.